


Neuromuscular scoliosis: diagnosis and treatment options

Priscila Cunha Santos
DHA License Number: 26093763-001
Senior Pediatric Physical Therapist
Neurology and Neuroscience, PhD

Children with progressive and non-progressive neurological impairment like cerebral palsy, muscular dystrophy, CDKL5 deficiency disorder, and myelomeningocele present abnormal and asymmetric muscle forces, which lead to inefficiency in performing functional tasks, pain, and increase the risk of developing neuromuscular scoliosis, which is an alteration of spine curvatures. Fortunately, these children can benefit from medical and rehabilitation programs that aim to reduce the curvature progression. Various treatment strategies can be adopted to that end.
Definition
According to the Scientific Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) in the third edition of their guidelines (Negrini, Donzelli, Aulisa et al., 2018), neuromuscular scoliosis is a general term referring to various conditions comprising changes in the shape and position of the spine, thorax, and trunk. It is generally described as a tri-dimensional spine misalignment that includes the extension, rotation, and inclination towards the same side of the vertebras in one or more spine segments.
“Structural scoliosis”, or just scoliosis, is different from “functional scoliosis”, which means a reversible misalignment (Negrini, Donzelli, Aulisa et al., 2018). “Structural scoliosis” includes mechanical adaptations of vertebras, discs, and rib cage that are not reversible.
Causes
Neuromuscular scoliosis is caused by various underlying diseases. Poor muscular control, muscle weakness or paralysis, and muscle overactivation or spasticity cause abnormal and asymmetric muscle forces in children, which make them unable to symmetrically maintain their spine under the force of gravity . These imbalances contribute to the development of functional scoliosis and can be exacerbated during the growth spurt, resulting in rapidly progressive curves and structural scoliosis (Wishart and Kivlehan, 2021).
Risk factors
There are multiple risk factors for the ongoing and rapid progression of spinal deformity in neuromuscular patients (Wishart and Kivlehan, 2021). Trunk muscle weakness, causing primary an increased forward rounding of the spine, called hyperkyphosis (Wishart and Kivlehan, 2021), is a strong predictor of scoliosis in children with neuromuscular impairment (Bertoncelli, Bertoncelli, Elbaum et al., 2018).
Furthermore, neuromuscular scoliosis is typically associated with pelvic obliquity, or a tilted pelvis. According to Senaran, Shah, Glutting, et al. (2006), hip dislocation may cause pelvic obliquity and initiate scoliosis while neuromuscular scoliosis itself can lead to pelvic obliquity and may increase the risk of hip dislocation.
Prognosis
Regardless of the underlying neurological causes, the results of a progressive neuromuscular scoliosis deformity are similar. According to Murphy and Mooney (2019), the deformity may be associated with difficulties in daily care, ambulation or sitting balance in those unable to walk and stand, and wheelchair positioning. Over time, if left untreated, the deformity may contribute to pain, alterations in skin integrity, as well as respiratory and cardiological complications.
Diagnosis
Parents of children with neurological impairment should be aware of typical signs of neuromuscular scoliosis. Difficulty keeping the head and trunk upright and straight, excessive use of one side of the body, uneven shoulders and pelvis, especially in sitting or standing positions, are all symptoms of scoliosis. Based on this, further medical investigations are required.
A pediatric orthopedic doctor specializing in the spine will diagnose neuromuscular scoliosis based on clinical and radiological exams. Usually, clinical screening for scoliosis involves clinical observation of truncal asymmetries in several positions, mainly against the force of gravity and flexibility tests (Figure 1a). It can also include the Adams forward bend test, where the child bends their head and trunk forward and we can observe a hump on one side of the rib cage and/or lumbar segment. These humps can be measured with an inclinometer called scoliometer. However, the proper positioning of the child for these tests is challenging if they are non-ambulatory or present severe muscle tonus disturbance, pelvic obliquity, hip displacements, or other lower limb deformities. In such cases, it is best to assess and monitor the child’s posture observationally through a sequence of standardized photos (Figure 1b).
 Figure 1: Flexibility and modified Adam’s test
Figure 1: Flexibility and modified Adam’s testPosteroanterior (PA) and lateral radiographs, are the imaging modality of choice for scoliosis and they are best conducted over children in a standing position to help assess the true effects of gravity on the spine (Jones, Saigal, Palasis, et al., 2019). For non-ambulatory children, weight-bearing in a seated position can be used (Berven and Bradford, 2002). Radiographs should show the entire spine, from the cranium to the pelvis, to identify possible causes such as pelvic unevenness or postural malalignment with rotation of the head to one side. Once radiographs are performed, Cobb angle and Risser index can be calculated and monitored with repeat radiographs. The Cobb angle measures the degree of side deviation of the scoliotic curve, and the Risser index is a scale of skeletal maturity. This information allows the doctor to establish the risk of progression of scoliosis and to decide on surgical or conservative treatment (Wishart and Kivlehan, 2021).
Treatment
The management of neuromuscular scoliosis includes either conservative or surgical treatment and depends on the Cobb angle, spine stability, the skeletal maturity, and any associated complications such as respiratory and cardiological dysfunctions. The decision for surgery is child-specific and should balance the risks and benefits related to the child’s quality of life.
Physiotherapy treatment of neuromuscular scoliosis aims to maintain the flexibility of the spine and rib cage and to correct or prevent the progression of hip dislocation, pelvic obliquity, and, consequently, of the scoliotic curve. Some scoliosis-specific physiotherapy treatment approaches, like Lyon and Schroth’s methods, are not appropriate for children with sensory, motor, cognitive and behavioral issues, which are commonly observed in cases of neuromuscular scoliosis. However, three-dimensional corrective alignment based on Lyon and Schroth methods’ mobilizations and positioning strategies are effective in such cases.
Postural management is an essential therapeutic strategy for neuromuscular scoliosis treatment that must be included in the child’s daily routine. According to Mehta (2005), by applying a constant external corrective force over time, it might be possible to make the scoliotic spine grow from a deformed into a regular shape. The earlier the treatment begins, the greater the chance of success. Postural care strategies focusing on the symmetric postural alignment should include prolonged positioning using a compression garment, dynamic orthotic suit or brace, an adapted wheelchair and corner chairs, a standing frame, and a therapeutic night or sleep positioning system.
In addition, children with neuromuscular scoliosis and multiple underlying deficiencies, including visual and other sensory issues associated with poor motor control, will need a broad interdisciplinary approach for successful scoliosis treatment. The interdisciplinary team will address all the components that lead to the asymmetrical postural alignment, especially during functional tasks and rest positioning, and plan the therapeutic strategies for the treatment.
Treatment outcomes
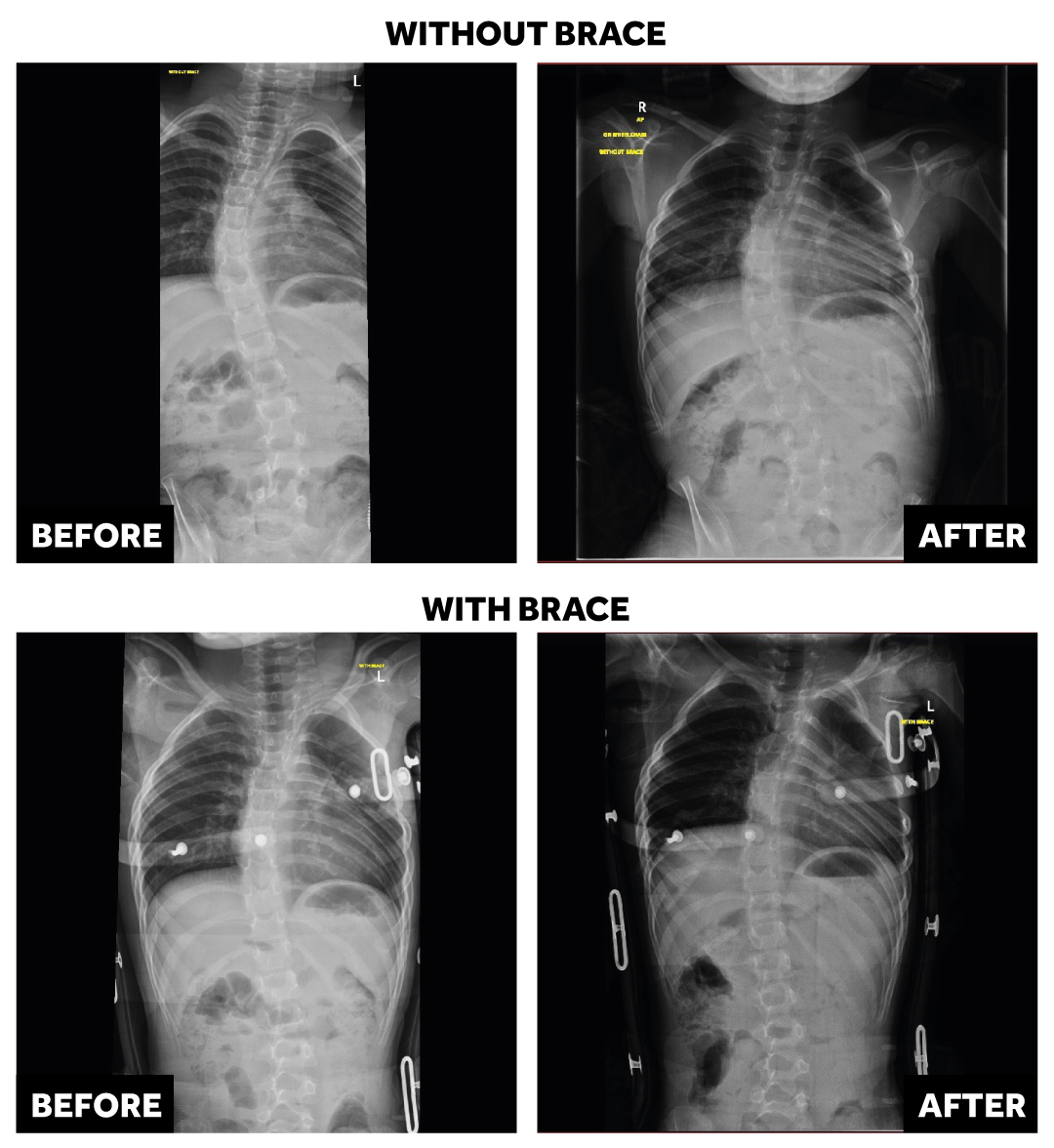
Outcomes in neuromuscular scoliosis are variable. A slight improvement or even no progression of the scoliotic curve is already considered a great outcome since neuromuscular scoliosis tends to worsen over time. In Figure 2 we can see an improvement in the scoliotic curve following five months of conservative and interdisciplinary treatment including a night brace.
Management plans require an interdisciplinary team that involves family and caregivers in decision-making. Family education is crucial as it highlights the possibility of curve progression despite therapy, positioning, and bracing (Wishart and Kivlehan, 2021). The rehabilitation team should focus on spine alignment, particularly during the child’s participation in daily routine tasks: at home, school, and in the community. The best outcomes of neuromuscular scoliosis treatment are the fruit of the joint work of the family, medical doctors, and the rehabilitation team.
High Hopes’ approach
The High Hopes team of physiotherapists is expert in identifying the symptoms of, monitoring, and treating neuromuscular scoliosis. Our focus is on promoting spine flexibility and pelvic, spine, and lower limbs alignment in children with progressive and non-progressive neurological conditions. Treatment strategies include interdisciplinary, functional, and playful activities, kinesiotherapy, vibration therapy, kinesiotape, suit therapy, Task-Specific Electrical Stimulation (TASES), and Schroth 3D Scoliosis Therapy. Our multidisciplinary team also provides recommendations on 24 hour-postural management that should be adopted at home and school settings.
Do not hesitate to contact us for more information or to book a consultation.
The month of June is observed as Scoliosis Awareness Month.
Sources:
- Negrini S, Donzelli S, Aulisa AG, et al. 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis and Spinal Disorders 2018;13:3. doi: 10.1186/s13013-017-0145-8.
- Bertoncelli CM, Bertoncelli D, Elbaum L, et al. Validation of a clinical prediction model for the development of neuromuscular scoliosis: a multinational study. Pediatr Neurol 2018;79:14-20.
- Wishart BD, Kivlehan E. Neuromuscular scoliosis. When, Who, Why and Outcomes. Phys Med Rehabil Clin N Am 2021. Article in Press. doi: 10.1016/j.pmr.2021.02.007.
- Jones JY, Saigal G, Palasis S, et al. ACR Appropriateness Criteria Scoliosis-Child. J Am Coll Radiol. 2019;16(5S):S244-S251. doi: 10.1016/j.jacr.2019.02.018.
- Berven S, Bradford DS. Neuromuscular scoliosis: causes of deformity and principles for evaluation and management. Semin Neurol 2002;22(2):167-78.
- Senaran H, Shah SA, Glutting JJ, et al. The associated effects of untreated unilateral hip dislocation in cerebral palsy scoliosis. J Pediatr Orthop 2006;26:769-772.
- Murphy RF, Mooney JF. Current concepts in neuromuscular scoliosis. Cur Rev Musculoskelet Med 2019;12(2):220-227. doi: 10.1007/s12178-019-09552-8.
- Mehta MH. Growth as a corrective force in the early treatment of progressive infantile scoliosis. J Bone Joint Surg Br. 2005;87(9):1237-47. doi: 10.1302/0301-620X.87B9.16124.