


Neuro-Developmental Treatment Approach: Do what works!

Kunali Doshi
DHA License Number: 00100771-002
Senior Pediatric Physical Therapist

What got me started?
I was first introduced to the Neuro-Developmental Treatment (NDT) Approach in the year 2006, when I was seeking knowledge in neuropediatrics that would give me a stronger base as a therapist in understanding children with special needs. By that point I had already worked in a pediatric clinic where I had the opportunity to treat children with varied diagnoses. That experience gave me a bird’s eye view of what my role as a physical therapist would be. I really wanted to cultivate my skills and develop my practice to provide each child and family with the best possible care.
The day I started my 2-month intensive NDT Basic course under Judith Bierman was an eye-opening moment for me. From that instant until today, NDT has given me a new perspective. I notice all the subtle details about the child’s alignment and the foundation of postural control. It is impossible to articulate all that NDT has given me, but three things stand out:
- An understanding of the very basis of analyzing atypical and typical posture and movement, and as a therapist, a starting point to identify where the child is struggling with movement.
- Therapeutic handling and my ability to use my voice, my body movement, and my hands to influence the child’s movement
- A clinical decision-making framework, to set child centered and family-oriented goals, considering the contextual factors of a child and the environment they function in.
The Inception of the NDT(Bobath) Approach
Dr. Karel Bobath and Mrs. Berta Bobath, Physiotherapist, introduced their model of therapeutic intervention in the 1940s, which for many years was simply called The Bobath Approach. At that time, Dr. Bobath described their intervention model as a living concept, aware that science and clinical practice would change some of the most basic assumptions without affecting the underlying idea: that change and recovery of function is possible for persons with neuromuscular dysfunction regardless of age or time of onset.
Beliefs and Viewpoint of NDT
NDT is a holistic and interdisciplinary clinical practice model informed by current and evolving research that emphasizes individualized therapeutic handling based on movement analysis for rehabilitation of children with neurological pathophysiology.
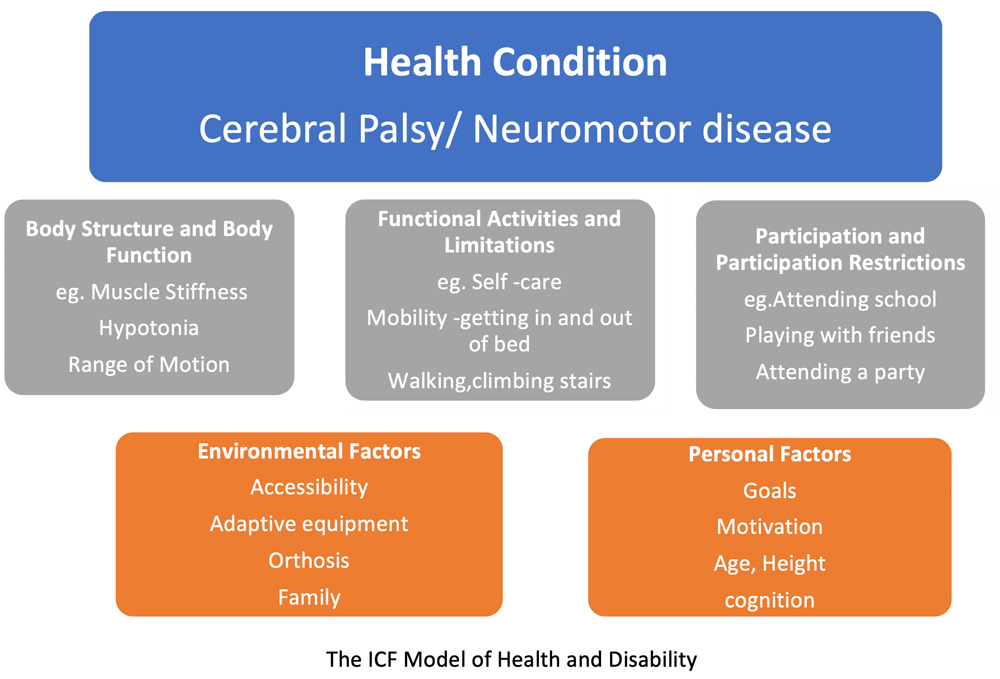
The therapist uses the International Classification of Functioning, Disability and Health (ICF) model in a problem-solving approach to assess activity and participation, thereby identifying and prioritizing relevant integrities and impairments as a basis for establishing achievable outcomes with clients and caregivers.
The basis of examination, evaluation, and intervention in NDT are formed by an in-depth knowledge of the human movement system, including the understanding of typical and atypical development, and expertise in analyzing postural control, movement, activity, and participation throughout the life span.
Therapeutic handling used during evaluation and intervention consists of a dynamic reciprocal interaction between the child and therapist, aimed at activating optimal sensorimotor processing, task performance, and skill acquisition to enable participation in real life environments and meaningful activities.
Do what works
- NDT provides me with a starting point in observing the child, to understand the how and why of movement dysfunction.
As Mary Quinton rightly said, “First train the outer eye to observe and record, then look with the inner eye to analyze the probable causes for what the outer eye sees.“ - NDT is a child-centric approach with emphasis on working on strengths of the child as an individual.
For example, a 3-year-old child with athetoid Cerebral Palsy who is unable to speak, but who has created and uses informal “sign language” that his family understands, is quite competent in getting his basic needs at home. - We focus on effective and ineffective posture and movement strategies and identify compensatory strategies used by the child during function. This involves assessing the child’s malalignments and compensations in one area which directly affects their movement and overall functional ability.
For example, a child with Cerebral Palsy develops a W-sitting pattern to avoid using the core muscles of the trunk, which leads to changes in the shin bone torsion with bony changes also at the hip joint. - The impairments are addressed in the context of the child’s goal in a functional setting.
For example, a child with hemiplegia needs to use the less-involved side for support when rising to stand; he cannot rise to stand while holding an object in his hand. - Handling encompasses therapeutic use of auditory input, visual input, movement of therapist’s body as well as hands on information.
For example, a Physical therapist would wonder, “Can little K get up to standing from her chair with less effort if I assist her weight shift forward? Or if I give her the feeling of pushing into the support, can she then do it without my assistance? Or will baby increase the amount of time reaching with outstretched arms with an audio-visual stimulation from a toy? Or if I provide proximal stabilization at her shoulders? - Intervention is designed to obtain active responses from the child in goal directed activities.
For example, M will get up from bench sitting to standing whilst holding on the grab bars of walker with verbal prompts. Or M will push her pants down from her hips, once started and seat herself on a regular toilet using a small step.
Active feed-forward movements guided by the therapist’s facilitation are effective in obtaining the desired outcomes for children who cannot participate in cognitively directed movements. - This approach provides a comprehensive understanding of the children we work with and helps me to collaborate with my OT and SLT colleagues to treat the child as an individual.
For example, in children with Cerebral palsy, the ribcage often remains elevated and spine rounded. This affects the mobility of the ribcage needed during movement and speech. Immobility of the laryngeal areas develops due to low tone or increased muscle tone and failure to develop an upright posture against gravity. - It is an approach that has evolved over a period of many years and continues to shift our paradigm in thinking.
What does the Future hold for NDT?
Technological advances in neurorehabilitation, such as robotics, exoskeletal systems, combined with the current techno-savvy generation do present cause of concern regarding the expectation of our future therapists and consequently the future and survival of this hands-on approach.
We are hopeful that as robotics become less expensive, therapists will see these means of providing additional practice opportunities for patients outside of therapy sessions rather than a replacement for valuable, skilled, quality one-to-one therapist to patient intervention.
Could technology provide us with more sophisticated measures of change in alignment, muscle activation, quality, and efficacy of movement, which are all hallmarks of NDT intervention but difficult to measure with any of our current standardized outcome measures?
If you are looking for a NDT certified therapist please feel free to contact Kunali Doshi on kdoshi@highhopesdubai.com for any guidance or consultation for your child.
Sources:
- Stamer M. Explaining NDT: A clinical practice model. NDTA Network. 2012;19:32-34
- Stamer M. Who owns the research? Theory vs Philosophy in NDT debate. NDTA Network 2006;13:9-10
- Howle J. Development of Bobath approach: Theoretical Foundations and Principles of Clinical Practice. Laguna Beach, CA: Neuro-Developmental Treatment Association;2002:315-370
- Karen Bruton, Neuro-Developmental Treatment: Research and Clinical Support for an Enduring Philosophy. NDTA Network 2018
- The International Classification of Functioning, Disability and Health model demonstrating the Health/Disability : ICF, Geneva, World Health Organization, 2002 (http://www.who.int/classifi cations/ icf/training/icfbeginnersguide.pdf, accessed September 8, 2014)